Iain Davis
UK Column
COVID-19 has been circulating for at least a year and yet there was no notable increase in unseasonable mortality anywhere until Lockdown regimes were imposed between late February and late March 2020. Let me repeat that: everywhere, the overall or “all cause” mortality data consistently tells the same story: there was no notable deviation from the statistical norm in any country until lockdown regimes were imposed.
According to the World Health Organisation (WHO), at the time of writing, with 11,841,326 supposedly confirmed cases and 544,739 alleged deaths, this is a global pandemic which has infected approximately 0.15% of the global population and has allegedly led to the deaths of 0.007%. This makes it slightly less deadly than a bad seasonal influenza which can kill 0.0085% of the world’s populace in a single year.
Yet governments around the world decided that the only way to respond to this particular respiratory infection was to roll out the most oppressive form of governance ever seen in the west, outside of a time of war.
The measures taken by our “elected representatives” have already killed many people and will prematurely end the lives of many more in the weeks and months ahead.
COVID-19 Arrived Long Before The Lockdown Regimes
I began this article with the claim that SARS-CoV-2 “has been circulating for at least a year”. The evidence for this statement has come from tests of sewage in multiple countries.
The Italian National Institute of Health (ISS) found SARS-CoV-2 in sewage samples collected on December 18th 2019 from Milan and Turin.
Two separate samples, gathered independently, from Brazilian wastewater showed the that the virus had been present in November 2019.
Researchers from the University of Barcelona found a number of samples indicating the presence of the virus in mid January 2020, 6 weeks before the Spanish Lockdown, with one sample dating as far back as March 2019, a year before any lockdown regimes were rolled out.
The science behind wastewater surveillance for SARS-CoV-2 is well established and, in April 2020, Australian researchers confirmed detection in wastewater as proof of concept for wastewater based epidemiology (WBE) for SARS-CoV-2. Further studies support its efficacy.
Prior to the release of these results, a systematic review of the available science on the possible faecal shedding of SARS-CoV-2 RNA found consistent evidence of the presence of SARS-CoV-2 in faecal matter. Looking at 26 relevant studies, researchers noted that nearly 54% of stool samples taken from confirmed COVID-19 patients contained SARS-CoV-2. They concluded:
There is a high rate of positive polymerase chain reaction tests with persistence of SARS‐CoV‐2 in faecal samples of patients with COVID‐19.
While knowledge gaps remain, the debate about WBE for SARS-CoV-2 is about how best to use it, potentially as a predictive tool for future outbreaks. There is little doubt that RNA from SARS-CoV-2 can be detected in sewage.
Consequently, it is the recorded dates of these samples which raises significant questions, not the scientific credibility of the sampling process.
The claims of so called fact checkers that no inference can be drawn from these sample dates, due to the likelihood of false positives, are specious.
Once found, the samples were tested with RT-PCR, the common test for SARS-CoV-2. Fact checker attempts to downplay the significance of these results, by citing possible false positives, also provides reason to question every other diagnosis of SARS-CoV-2 infection with RT-PCR — the predominant testing method upon which every lockdown regime is based.
There has been some resistance to accepting the growing evidence that SARS-CoV-2 had already spread across continents long before the WHO declared a global pandemic. Claire Crossan, research fellow in virology at Glasgow Caledonian University, explained:
A curious thing about this finding is that it disagrees with epidemiological data about the virus. The authors don’t cite reports of a spike in the number of respiratory disease cases in the local population following the date of the sampling.
This evidence runs contrary to all that we have we have been told about COVID-19. Crossan was right to observe that Spanish, Brazilian and Italian results did not correspond to any known outbreak of the associated COVID-19 syndrome. This is no reason to discard this evidence, but it does provide grounds to question the prevailing COVID-19 narrative.
No Pre-Lockdown Mortality
Due to the quite remarkable debasement of normal death registration procedures in England and Wales, under the 2020 Coronavirus Act, it has become virtually impossible to identify cause of death within the resulting statistics.
It is, however, much harder to politicise total numbers of deaths. By looking at all cause mortality, despite all the COVID-19 fear porn pumped out by the MSM, it is possible to reach a relatively accurate analysis.
In his recent technical report Denis Rancourt Ph.D, former Physics professor at the University of Ottawa, highlighted this problem:
…It is difficult to interpret the synchronicity of the WHO declaration of COVID-19 as a pandemic and the onset of the observed surge in reported COVID-19 cases and deaths as being the product of either coincidence or [the] extraordinary forecasting ability of the global health monitoring system. Instead, in light of past epidemics, it is more likely that this remarkable synchronicity phenomenon arises from biased reporting…That is why rigorous epidemiological studies rely instead on all-cause mortality data, which cannot be altered by observational or reporting bias (as discussed in Simonsen et al., 1997; and see Marti-Soler et al., 2014). A death is a death is a death.
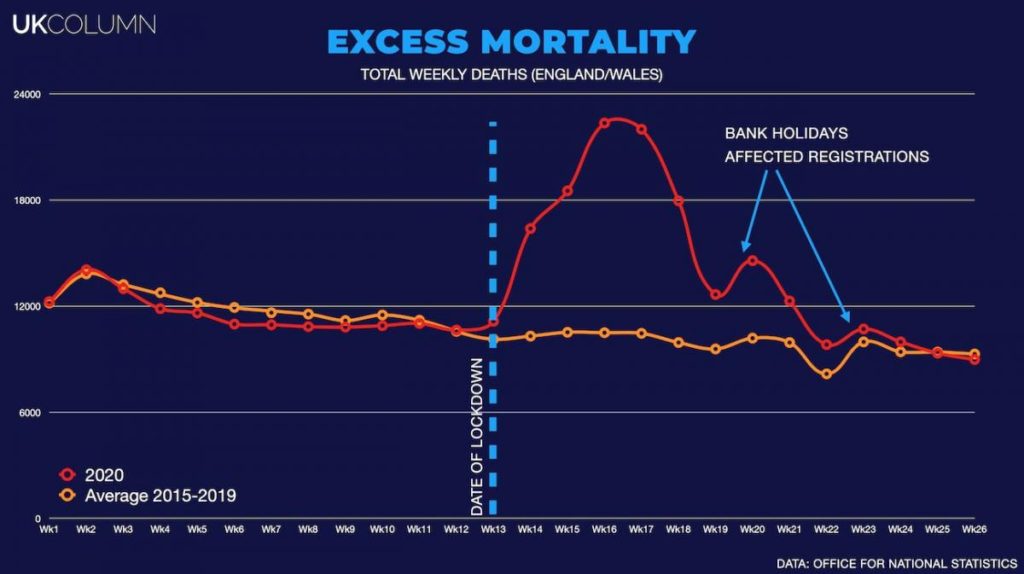
When weekly deaths for England and Wales, covering the last decade, are plotted we can see that all cause mortality has been broadly consistent. Every winter sees an increase, as mortality rises sharply during the colder and less humid winter months.
Respiratory like illness, such as flu, pneumonia and SARS, are diminished by increased summertime humidity. Consequently the mortality risk, especially for those with severe comorbidity, such as cardiovascular disease and cancer, increases in the winter.
If we plot the deaths on a weekly bases the incline of the peak shows the death rate. That is, the more people who die per week, the higher and sharper the spike appears. The total number of deaths are represented by the area beneath the peaks. So a very high but narrow spike in mortality does not necessarily mean that an unusually large number of people have died. It suggests something caused people to die in a distinct cluster.
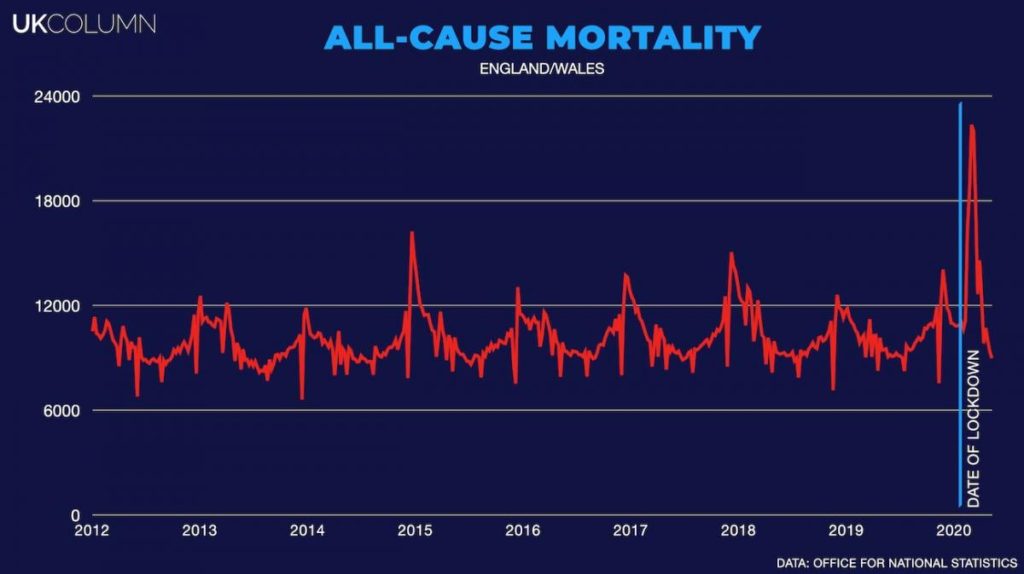
If we look at the last 10 years of all cause mortality data for England and wales, two facts are evident:
- people have died at a significantly increased rate over a very short timescale in 2020
- a mortality spike occurred much later in the year than has been observed in previous years
These marked statistical features are nearly identical for all lockdown countries.
The first cluster of COVID-19 cases supposedly emerged in China in December 2019, though it had already made its way to Italy, Spain and Brazil by then.
Initial cases in the U.S. were seen in late January with the first death recorded on February 6th.
The first outbreak reported cluster occurred in Italy in early February and community infection in Spain was underway by mid February.
The UK saw its’ first confirmed case in January and person to person transmission had also emerged by early February.
New Zealand and Australia reported cases in late February, as did Brazil.
From the official Wuhan outbreak it supposedly took just 9 weeks for SARS-CoV-2 to spread around the world. With the symptoms typically emerging between 5-6 days post infection, COVID-19, and associated mortality, closely followed the spread of the virus.
The WHO declared a global pandemic on the 11th of March. If the hope was to stop SARS-CoV-2’s global contagion, we now know this was a rather belated effort. If the speed of transmission is as we are told, then it had already spread around the world by December 2019, at the latest.
A pandemic shouldn’t be a political decision, it should be an evident reality. As I have shown above, the increasing body of evidence demonstrating that SARS-CoV-2 was in circulation at least at the beginning of the normal flu season, raises the question of why it took months for anyone notice COVID-19 in Italy, Spain, Brazil or the UK?
If COVID-19 is responsible for the spikes in mortality which have been seen from March until June, why did SARS-CoV-2 wait until lockdowns were implemented to begin killing people?
Viruses don’t pander to the whims of policy think tanks and no one, anywhere, had implemented any stringent measures, either to control the spread or mitigate the health risk of COVID-19, until lockdowns were stamped into existence. The virus was free to do its thing for months and yet it apparently did nothing.
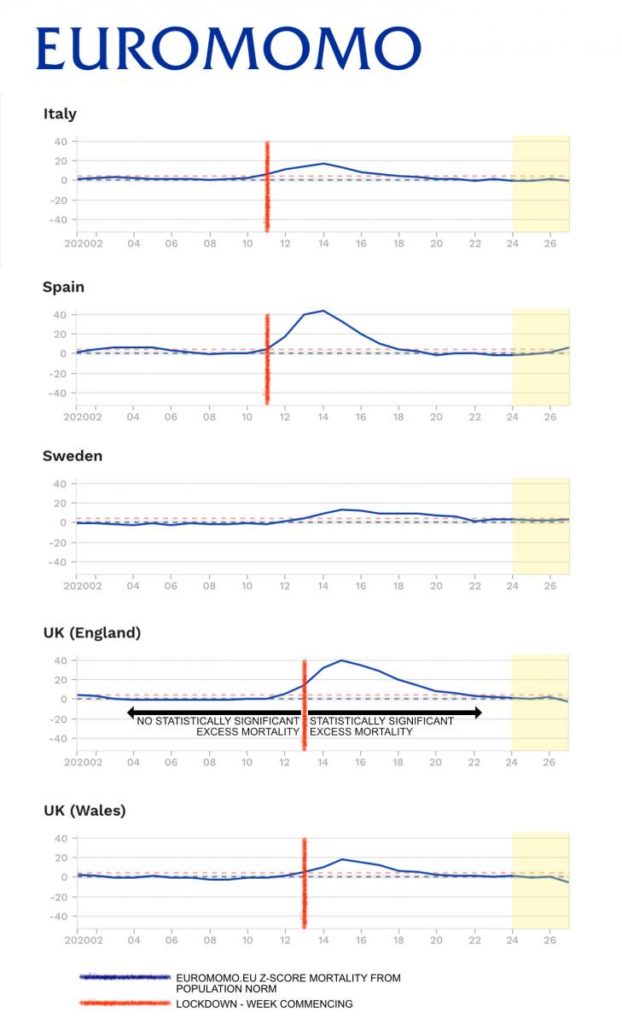
In both England and Wales, the lockdown marked the statistical boundary between ‘no significant’ and ‘observed significant’ excess mortality.
While no policy maker had any idea that the virus had been in circulation for months, their attempts to “flatten the curve” accurately predicted the onset of rapidly increasing mortality with uniform precision in every country. How could they have known that their lockdown regimes would be so perfectly timed to “flatten any curve?”
Targeting The Most Vulnerable
For this article, I will primarily discuss the Lockdown regime in England and Wales. However, the same issues I will raise here can be found wherever the lockdown hammer fell.
It is generally recognised that the vast majority of those who have died with COVID-19 had at least one serious comorbidity and were over 65 years old with more than 83% over 70. The deaths have occurred almost exclusively among those who were approaching, or already receiving, end of life care.
Their deaths were precipitated either by a latent virus which only became active once the political class were ready for it, or by the health consequences of the political response to the WHO’s declared “global pandemic.”
If the intention was to protect the most vulnerable, then many Lockdown regime policies and decisions were, at best, criminally negligent. In combination, they appear to be suspiciously close to a deliberate program of euthanasia.
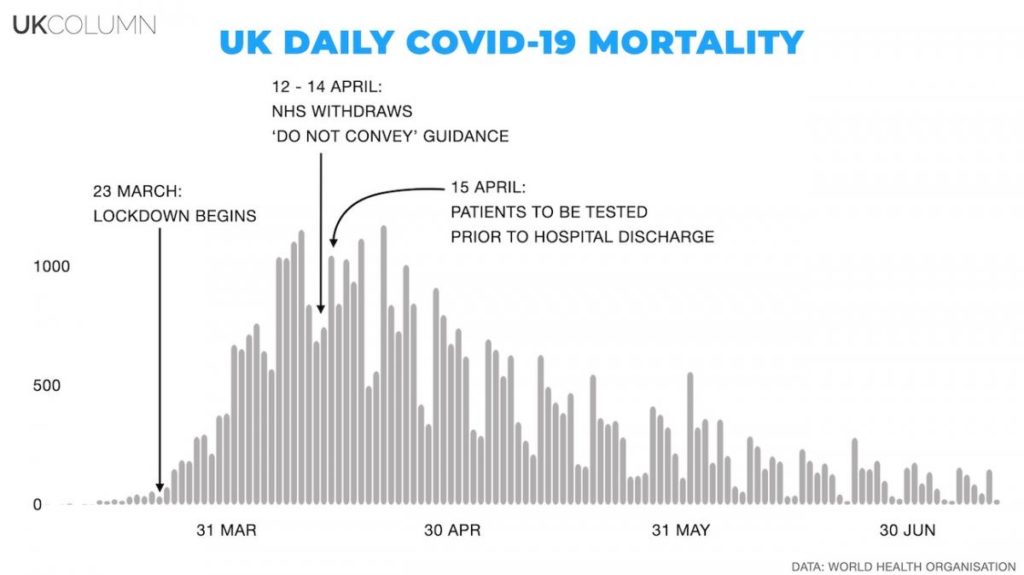
The mortality spike in England and Wales peaked between 9 – 12 April. It was at this time that NHS England withdrew their “do not convey to hospital” guidance.
Prior to this withdrawal, as a result of early lockdown policies put in place in order to “protect the NHS,” NHS England decided not to allow specified groups of vulnerable patients to be admitted to hospital. This meant not treating those over the age of 70, who displayed normal vital signs, and any who had supposedly elected not to be resuscitated, regardless of their health condition.
At the same time the government and the NHS were pressurising vulnerable older people to sign “do not attempt resuscitation” (DNAR) notices. Amid all the propaganda about how important it was to protect the NHS, vulnerable people were sent DNAR notice agreement forms through the post (my elderly father received one) and there were numerous reports of these being completed en masse without the older persons consent in care settings, automatically excluding vulnerable people from hospital treatment.
Further, the guidance advised that vulnerable people should not be taken to Accident and Emergency departments unless approved by a clinical adviser, thereby increasing the delay in treatment during the vital golden hour. This caused considerable concern amongst health professionals.
In order to “manage” the potential dissent, it has become increasingly apparent that UK NHS staff are subject to strict gagging orders. Those who have spoken out are either retired or have done so anonymously.
For example, speaking about the introduction of an additional “clinical adviser” into the golden hour window, an anonymous senior NHS leader spoke to the Health Service Journal:
[The policy is] prejudiced against older people, those with dementia and those in care homes. [It risked placing] obstacles between vulnerable older people and emergency departments (ED’s), [and would put] significant burdens on systems not equipped to provide pre-ED 24/7 expert clinical advice. This raises serious questions about the origins of the guidance, its clinical rationale and the level of scrutiny and consultation it underwent prior to publication.
Correlation doesn’t equal causation but, nonetheless, this specific guidance was withdrawn at the same time that mortality peaked and the death rate began to fall. We shouldn’t simply discard this correlation. It is one among many.
The demands of the lockdown regime also saw ambulance response times increase significantly. Most notably in London, where they more than trebled for the most seriously ill “category 2 patients,” including heart attack and stroke victims.
During the peak of the outbreak 9 out of 10 of the local authorities with the highest mortality rates were London boroughs. Presentations to Accident and Emergency departments (ED’s) were down by 50% in London and the average drop in A&E attendance was down by 53% nationally during the lockdown.
Cancer screening and treatment was put on hold. Cancer Research UK estimated that 290,000 people missed cancer follow ups, indicating that around 20,000 current cancer sufferers, who could otherwise have accessed treatment, remain untreated or possibly unaware of their cancer.
At least 2.4 million people missed cancer screening appointment during the lockdown. As the the NHS Confederation warns that the backlog of planned treatments, including for life threatening and life limiting conditions, is likely to hit 10 million, the Lockdown regime has also seen cancer referrals drop by 45%. Some scientists have estimated this could mean an additional 35,000 excess cancer deaths in the UK.
There were no fewer people contracting cancer, but the real world impact of the Lockdown regime is that fewer lives will now be saved while many have undoubtedly already been lost. We are currently inundated with warnings of future lockdowns and local UK lockdowns have already begun in Leicester.
Many people are already living in fear of the alleged threat of the second COVID-19 wave. Consequently, they are willing to comply with any diktat from the government, regardless of scientific justification or lack of it.
It is extremely difficult to envisage how health services will manage the enormous treatment backlog and many health professionals are warning of the likelihood that they won’t. As winter approaches and natural mortality increases, the pressure on services will be immense. Another large spike in mortality in the Autumn is a terrible but seemingly unavoidable prospect. Given what we already know about the appalling manipulation of the death registration process, we can only guess how many of these deaths will ultimately be attributed to the second wave of COVID-19.
The Lockdown regime’s impact upon those with cardiovascular disease and heart conditions has been equally deleterious. Patients report difficulty accessing treatment or even obtaining the vital medication they need. Dr Sonya Babu-Narayan, Associate Medical Director of the British Heart Foundations, said:
People with heart and circulatory diseases are already at increased risk of dying from Covid-19 … At the very least, around 28,000 planned inpatient heart procedures have been deferred in response to the Covid-19 outbreak in England alone … If hospital investigations and procedures are delayed too long, it can result in preventable permanent long-term complications, such as heart failure.
The pervasive nature of our collective delusion is notable. Even renowned heart specialists seem incapable of acknowledging the truth. Heart disease is the most common comorbidity allegedly contributing to deaths with COVID-19.
During the lockdown, A&E presentations for heart attacks and strokes dropped by more than half. This resulted in a huge increase of deaths in the home.
It wasn’t COVID-19 that killed the majority of these people. They lost their lives because they either couldn’t or wouldn’t access hospital treatment.
The most vulnerable were sent letters telling them to stay at home to “protect the NHS;” ambulance response times increased; access to hospital treatment was actively deterred and community healthcare was withheld. This was not “because of coronavirus” or even “due to the response.” It is the result of a vicious Lockdown regime.
It is ludicrous to imagine that the cumulative effect of these lockdown policies didn’t lead to early mortality among the most vulnerable. The lockdown regime was detrimental to the health of the very demographic it was supposedly designed to “keep safe.”
While there is no evidence that COVID-19 presents any risk to children, there is evidence that the Lockdown regime does. A&E presentation were also down for children, raising concerns they they have not been receiving the health care they need.
Regardless of the MSM’s unrelenting assertion that these problems are caused by coronavirus, it has been the Lockdown regime’s policies, coupled with the MSM’s omnipresent fear porn, that has deterred frightened parents and increased the health risks for children.
The level of MSM disinformation during the lockdown has been staggering. For example, without questioning or verifying anything, they carelessly reported claims of massive underestimates of COVID-19 death in care settings. Closer analysis of those figures revealed these assessments were based upon little more than assumptions. In reality, the vast majority of those claimed coronavirus deaths were not related to COVID-19.
We should remember this as we consider the huge impact of lockdown regime policies on the most vulnerable people in society: those in care and nursing homes, and those who require home care.
Professor Carl Heneghan observed:
In order to free up space in hospitals, older patients were discharged into care homes without even being tested for the virus. In the two weeks after lockdown, when the risk of infection should have been waning, a further 1,800 homes in England reported outbreaks.
Once again, another notable correlation is evident. With its ever changing, bewildering policy guidance, it was on 15 April, immediately following peak mortality, that the UK government changed its recommendation to the NHS and stated that all patients must be tested for SARS-CoV-2 prior to discharge from hospital.
However, while every relatively healthy person, for whom COVID-19 presents virtually no threat, will be forced into quarantine for 14 days if they are even suspected of being in contact with someone who may have SARS-CoV-2, that same degree of caution does not apply the the most vulnerable. The current guidance states:
A small number of people may be discharged from the NHS within the 14-day period from the onset of COVID-19 symptoms needing ongoing social care. They will have been COVID-19 tested and have confirmed COVID-positive status. Some care providers will be able to accommodate these individuals.
Having sent an unknown number of infectious people into the care system, the UK government issued lockdown regime guidance to care staff recommending that they should not provide any care without the necessary personal protective equipment (PPE). The same policy makers then neglected to provide access to that PPE. As a result, the mounting stress and anxiety of care staff exacerbated the furlough staffing crisis.
Many staff members in nursing homes are medically qualified, this is not the case in the majority of care homes or among those providing community care. They are reliant upon primary care advice and intervention from their local GP.
The lockdown regime virtually removed GP support from care settings and the community. People have had to get used to telephone consultations instead of examinations and home visits. Thereby, hugely increasing the risk to the most vulnerable in the middle of an alleged global pandemic.
Guidance to GP’s from NHS England stated that possible COVID-19 patients should be identified primarily by weekly check-ins online. This was in keeping with the NHS Key Principles of General Practice, in relation to COVID-19, which stated:
Remote consultations should be used when possible. Consider the use of video consultations when appropriate.
Care home providers repeatedly highlighted the lack of medical care, as they struggled to cope with the condition created by the Lockdown regime. Despite representatives from the medical profession claiming that not providing medical interventions during a pandemic was “sufficient,” Vic Rayner, executive director of the National Care Forum, observed:
We are not focusing enough attention at a medical level on how best to keep people safe in these environments. We always knew these were the most at-risk groups, but we haven’t responded to an unprecedented situation with an unprecedented plan as we did in hospitals.
The UK government’s, or any government’s, claim that their ongoing Lockdown regime is intended to “protect the most vulnerable” is not credible. The consistency with which lockdown policies have increased, rather than reduced, the risk to those most in need has been a common feature of every lockdown.
Simultaneously, every Lockdown regime has placed those not at risk under ever more authoritarian rule. Quarantining the healthy is yet another Lockdown regime policy which escalates the risk for vulnerable people.
While the vulnerable were being sent back into high risk, poorly protected and understaffed care homes, hospital bed occupancy, across the country, was at a record low.
Whether by design or criminal neglect, lockdown policy has actively targeted the most vulnerable, singling them out for unusual and cruel treatment. Premature mortality is the inevitable and obvious result.
Lockdown Deaths Not COVID Deaths
We have clear evidence that the Lockdown regime has caused, and will continue to cause, ill health and death. We also know that it is likely that SARS-CoV-2 had already spread around the world before any lockdowns were initiated. We also know that the virus lay virtually dormant and only decided to cause statistically significant mortality after the lockdowns began.
We can now add the observations that the harshest elements of the lockdown, namely the refusal to allow care and the dispatching of untested vulnerable people back into high risk communities, only relented as peak mortality began to wane. We can also see, as lockdown restrictions eased, so did the mortality rate.
Nothing discussed here suggests that there is no virus or that COVID-19 doesn’t present a threat to health. It suggests that if your response to a public health crisis is to withdraw healthcare from those who need it the most, a spike in mortality is the only possible outcome. Not only are those affected by the disease more likely to succumb to it, but increased mortality from every other comorbidity is hard wired into that lockdown policy.
This would seem to account for the strong correlation between the imposition of healthcare limiting lockdowns and sharp increases in mortality. We can postulate that, prior to this, the virus was causing some mortality within the normal range and distribution of seasonable respiratory illness. Once the WHO identified the “novel” virus and declared a global pandemic, it was the ensuing Lockdown regimes which prompted unseasonable spikes in mortality. This was then attributed to a newly discovered disease that had long been present.
Italy’s National Institute of Health (ISS) found that only 12% of reported COVID-19 deaths were actually attributable to the COVID-19 syndrome. Perhaps this explains why another aspect of many Lockdown regimes has been the creation of indecipherable mortality recording systems.
The immediate response will be that this is a circular argument. The Lockdown Regime responded to the conditions on the ground. Policies adapted to circumstances at the time. As mortality reduced some restrictions could be lifted. If lockdowns cause mortality then why is a similar pattern found in a non lockdown country like Sweden?
While Sweden didn’t adopt the economic shutdown favoured by other European states, it did operate a policy of socially isolating the most vulnerable in poorly staffed, overcrowded care homes. Swedish care homes have been in a staffing crisis for many years, and this problem was compounded by the Swedish decision to tell all staff, who had any symptom ranging from a headache to a stiff knee, to stay at home. High mortality in the Swedish care system is an established problem and seasonal flu mortality in Swedish care homes is appallingly high.
The MSM, desperate to justify their own national lockdown regimes on behalf of their partners and leading advertisers, the government, have used Sweden’s high mortality in care homes as a stick to beat them with. In reality, instead of MSM propaganda land, around 50% of all recorded COVID-19 deaths across Europe, including in the UK, have been in care settings.
Sweden has openly admitted its error. Lena Hallengren, Swedish Health and Social Affairs Minister, stated in a national television interview:
We failed to protect our elderly. That’s really serious, and a failure for society as a whole. We have to learn from this, we’re not done with this pandemic yet.
It remains to be seen if Sweden will address the systemic failings within it’s care sector. Meanwhile Lockdown Regimes around the world persist with the lie that abandoning those most in need will “save lives.”
In light of all the other factors we have discussed, it is reasonable to conclude that the majority of deaths reported as COVID-19 mortality, by the world’s mainstream media (MSM), were not attributable to the syndrome itself, but rather to the various national and statewide lockdown policies.
These were Lockdown regime deaths not COVID-19 deaths. By restricting access to health care for the most vulnerable, any claim that Lockdown Regimes save lives is patently absurd.
This story was originally published at UK Column.org.
READ MORE COVID-19 NEWS AT: 21st Century Wire COVID Files
SUPPORT OUR INDEPENDENT MEDIA PLATFORM – BECOME A MEMBER @21WIRE.TV